
Summits | Meetings | Publications | Research | Search | Home | About the G7 Research Group
Follow @g7_rg

|
Summits | Meetings | Publications | Research | Search | Home | About the G7 Research Group Follow @g7_rg |
|
Can International Law Improve Compliance with G7 and G20 Health Commitments?
Lauren Millar, Senior Advisor, G7 and G20 Research Groups
July 21, 2020
I am grateful for the data and analysis provided by members of the G7 and G20 Research Groups.
The Group of Seven (G7) major market democracies and the Group of 20 (G20) systemically significant states are both soft law bodies made up of countries and international organizations whose leaders meet regularly at summits, where they agree on consensus-driven commitments on a broad range of subjects. Can compliance with the commitments they make specifically on health be improved by invoking the hard law instruments of international regulations and conventions? This question is now of acute importance as COVID-19's exploding death toll continues to add to the already massive victim count from infectious and chronic non-communicable diseases worldwide. Yet the global health system, with the World Health Organization (WHO) at its core, is equipped with only two legal instruments: the longstanding International Health Regulations (IHR) and the more recent Framework Convention on Tobacco Control (FCTC). As a result, the G7 and G20 have been thrust to the centre of global health governance at the summit level, most notably with the G7's emergency summit on March 16, 2020, and the G20 extraordinary summit ten days later on March 26. How well have these two soft law summit systems used the existing hard law instruments to add legal force to the unique political authority their leaders and thus their summit have?
To provide an analytically sound, evidenced-based answer, this study first examines the health commitments made by the G7 summits since their start in 1975 and by the G20 summits since they began in 2008, to see how often their leaders have invoked international law. It then examines members' compliance with these commitments to see if such compliance is higher with those that invoke international law than with those that do not. As the first systematic investigation of this subject using the most recent and robust databases, this study contributes to the ongoing hard law–soft law debate in international relations, suggests how G7 and G20 health compliance can be improved, and provides a foundation for urgently needed further research.
This study finds that the G7 has very rarely used hard law and seldom used soft law in its commitments. Invoking international law seems to improve compliance, but it is only soft law in the G7 that does so. The G20 seems to use hard international law proportionally more than the G7. Yet the compliance impact of both hard law and soft law remains unclear. The one clear message that emerges at this stage of the research is that G7 leaders should invoke soft law more often to improve compliance with the health commitments they make.
Global health law is unique in that it represents a largely decentralized legal system made up of a complex web of legally binding and non-binding regulations, agreements, declarations, strategies, action plans, programs and commitments.
Binding agreements are often referred to as hard law (Kirton and Trebilcock 2004; Kirton with Madunic 2009). In health they feature the mandatory IHR adopted and revised by the WHO (Kirton 2009; Kirton, Roudev and Sunderland 2007). The IHR is a legal framework that details the rights and obligations of WHO member states in handling threats to global health security, such as a cross-border public health emergency (Fidler and Gostin 2006; Lee 2009, 17–18). They also enable the WHO's World Health Assembly to adopt conventions or agreements with a two-thirds vote (Gostin and Sridhar, 2014). The FCTC is the first and only WHO convention that created legal rights and duties, and came into force in 2003 (Gostin and Sridhar 2014; Lee 2009, 94–95).
In contrast, soft law commitments such as global action plans or guidelines are non-binding in public international law. They are very common in the sphere of global health law (Lee 2009, 87–94). Although these instruments create non-binding norms, they may also trigger hard law in specific circumstances (Gostin and Sridhar 2014).
Some scholars theorize that bodies such as the G7 and G20 are soft law institutions for several reasons. First, their member governments tend to be averse to litigation. Invoking hard law mechanisms in G7 or G20 commitments could thus lead to unpredictable repercussions domestically (Gostin and Sridhar 2014). Furthermore, wealthier countries may be more hesitant to provide financing or commit fully to specific initiatives without fixed earmarks (Gostin and Sridhar 2014).
However, studies have shown that compliance can increase when there is a catalyst embedded in the text of a commitment that provides direction for implementation, for example a reference to a relevant core international organization such as the WHO (Hospedales et al. 2011; Kirton and Bracht 2015; Kirton and Fitzgibbon 2014; Kirton and Dobson 2020). These references to the WHO can be read as soft law health commitments. As such, G7 and G20 commitments that reference hard or soft law can test the hypotheses that "hard law instruments of formal rules contained in international law help members comply with their soft law summit commitments made at the hard law UN, while the core international organization that underscores hard law does so at the soft law G7" (Kirton, Knight and Hospedales 2018).
Between 1975 and 2018, G7 summits made a total of 418 health-related commitments (Muhanna 2019). Eleven of these commitments, or only 3%, referred specifically to hard law instruments.
The G7 Research Group assessed G7 members' compliance with 71 (17%) of these 418 health commitments. Compliance averaged 76%.
One assessed commitment explicitly referenced hard law and 23 explicitly invoked soft law.
The one hard law commitment assessed averaged compliance of 69%. In contrast, the 23 soft law commitments averaged compliance of a much higher 80%. Thus, invoking hard international law seems to reduce compliance, but using soft international law somewhat increases compliance.
In the newer, bigger, broader, more diverse G20, leaders made 75 health commitments between 2008 and 2018 (Warren 2019). Six (8%) referenced hard law and 18 (24%) referenced soft law.
Of these 75 health commitments, 11 have been assessed for compliance by the G20 Research Group. They averaged compliance of 69%. Only one explicitly referred to soft law, in the form of a reference to the WHO, and none referred to hard law. The one that referenced soft law averaged compliance of 65%, or 4% less than the average compliance of all.
This database shows that the G20 has used hard international law proportionally more than the G7. Its impact on compliance remains unknown (see Figure).
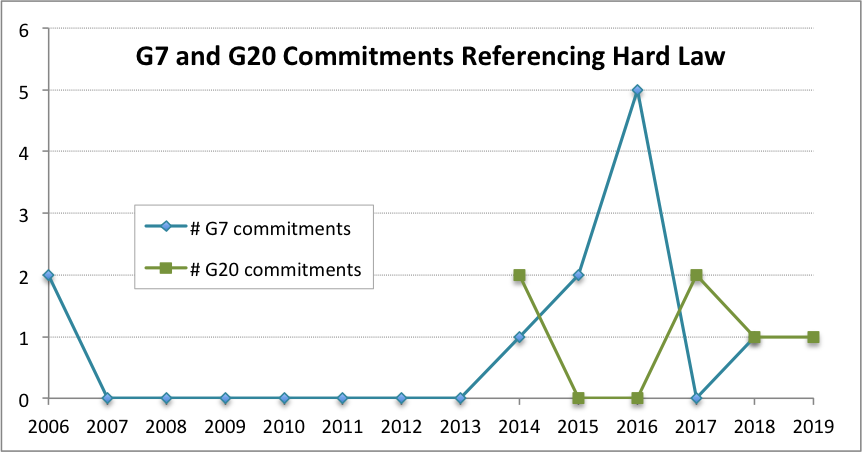
Both the G7 and G20 had years where commitments with hard law spiked. At the G7's Japanese-hosted Ise-Shima Summit in 2016, there was a spike to five hard law commitments. In the G20, such spikes occurred at the Australian-hosted Brisbane Summit in 2014 and the German-hosted Hamburg Summit in 2017.
The G7 spike in hard law commitments in 2016 can largely be attributed to its invocations of the WHO's IHR. This was due to the outbreaks of Ebola and Zika, which underscored the need for an emphasis on global health security.
The language used in these hard law commitments tended to be stronger than that in soft law commitments, or in commitments that made no reference to legal instruments. Phrases such as "comply with" were common in commitments that refer the IHR.
The most recent G20 summit was held an extraordinary one by video conference on March 26, 2020. Leaders made 47 commitments overall. They included 22 (47%) core health commitments (commitments directly focusing on issues of health) and a further six 13% health-related ones (commitments that referred to health as an instrument, condition or co-benefit, such as those referring to occupational health and safety or health-environment links), for a total of 28 (58%) with health content overall.
Only one core health commitment referred to international law. It was to the hard law of the IHR. It read: "We will … strengthen health systems globally, including through supporting the full implementation of the WHO International Health Regulations (IHR 2005)" (G20 2020). Compliance with this commitment is currently being assessed. The results will be compared with the low compliance average of 63% on the four fully assessed core health commitments thus far, and the preliminary 80% compliance for a fifth assessed core health commitment "to work together to … strengthen scientific international cooperation." The 66% average for the five core health commitments is below the 69% average for all 11 assessed core health commitments from 2008 to 2018.
Invoking hard law in the G7 or G20's core health commitments does not seem to raise compliance with them, in the limited data available thus far. However, in a COVID-19 world, countries may be under increased scrutiny regarding their compliance with the hard law IHR pandemic preparedness and response regulations. In 2005, the pandemic of severe acute respiratory syndrome led to the revision of the IHR, and in 2016 the Ebola pandemic led to a spike in G7 hard law health commitments in 2016 (Gostin and Sridhar 2014; Dobson and Kirton 2020). Similarly, the G7 and G20 members may once again turn to the WHO and IHR to guide the world through this latest pandemic. This will undoubtedly be complicated by the recent decision of the United States to withdraw from the WHO, especially with the organization already struggling for donors as a small group of countries contributes 80% of its total budget (Gostin and Sridhar 2014). The long-term impact of this announced withdrawal on future compliance has yet to be seen.
The current global pandemic will likely also see a rise in soft law commitments. This happened in the case of the hybrid Pandemic Influenza Preparedness Framework, which blended soft law with binding obligations in 2011, in response to the H5N1 influenza outbreak then (Gostin and Sridhar 2014).
Overall, a lack of compliance data makes it difficult to make definitive observations regarding G7 or G20 members' compliance with their leaders' soft and hard law commitments. Yet previous research shows that including a reference to the WHO in G7 commitments increases compliance with them (Kirton, Roudev and Sunderland 2007; Kirton and Dobson 2020). There is thus reason to believe that references to soft and hard legal mechanisms create a greater sense of responsibility and accountability, particularly when paired with specific targets and definitive timelines for compliance. Furthermore, it is possible that more attention and stricter timelines for compliance will emerge in the ongoing COVID-19 world. Ideally, these commitments will reference the hard law IHR and such soft law instruments as those addressing pandemic outbreaks. This combination will support countries that struggle to fulfill their global health security obligations and in turn will increase overall compliance and save many lives.
Fidler, David P. and Lawrence O. Gostin (2006), "The New International Health Regulations: An Historic Development for International Law and Public Health," Journal of Law, Medicine and Ethics 34(1): 85–94. https://doi.org/10.1111/j.1748-720X.2006.00011.x.
G20 (2020). "Extraordinary G20 Leaders' Summit: Statement on COVID-19." Videoconference, March 26. http://www.g20.utoronto.ca/2020/2020-g20-statement-0326.html.
Gostin, Lawrence O. and Sridhar, Devi (2014), "Global Health and Law." Georgetown Law Faculty Publications and Other Works, 1338. https://scholarship.law.georgetown.edu/facpub/1338.
Hospedales, C. James, T. Alafia Samuels, Rudolph Cummings, Gayle Gallop and Edward Greene (2011), "Raising the Priority of Chronic Noncommunicable Diseases in the Caribbean." Revista panamericana de salud publica 30(4): 393–400. https://iris.paho.org/handle/10665.2/9507.
Kirton, John and Caroline Bracht (2015), "Explaining Compliance with Regional and Global Summit Commitments: CARICOM, UN, G8 and G20 Action on Non-Communicable Disease," Paper presented at the annual convention of the International Studies Association, New Orleans, February 21. http://www.g7.utoronto.ca/scholar/kirton-bracht-isa-2015.pdf.
Kirton, John and Joy Fitzgibbon (2014), "Examining the Success of Summits from the Sub-regional to Global Level: Nutrition and Non-Communicable Disease," Paper presented at the annual convention of the International Studies Association, Toronto, March 27.
Kirton, John and Michael J. Trebilcock, eds. (2004), Hard Choices, Soft Law: Voluntary Standards in Global Trade, Environment and Social Governance (Aldershot: Ashgate).
Kirton, John and Sonja Dobson (2020), "Putting Humanitarian Health First: G7 Summit Health Performance, 1975–2020." G7 Research Group. http://www.g7.utoronto.ca/evaluations/dobson-kirton-putting-humanitarian-health-first.pdf.
Kirton, John with Jelena Madunic, eds. (2009), Global Law (Farnham: Ashgate).
Kirton, John, Andy Knight and James C. Hospedales, (2018), "Implementing Global Summit Commitments on Health." Paper presented at the annual convention of the International Studies Association, San Francisco, April 2. http://www.g7.utoronto.ca/scholar/kirton-knight-hospedales-2018.html.
Kirton, John, ed. (2009), Global Health (Farnham: Ashgate).
Kirton, John, Nikolai Roudev and Laura Sunderland (2007), "Making G8 Leaders Deliver: An Analysis of Compliance and Health Commitments, 1996-2006," Bulletin of the World Health Organization 85: 192–99. https://www.who.int/bulletin/volumes/85/3/06-039917.pdf.
Lee, Kelley (2009), The World Health Organization (WHO) (Aldershot: Routledge).
Muhanna, Duja (2019), "G7 Performance on Health," in John Kirton and Madeline Koch, eds., G7 France: The 2019 Biarritz Summit (London: GT Media), pp. 40–41. https://www.globalgovernanceproject.org/g7-performance-on-health/.
Warren, Brittaney (2019), "G20 Performance on Health," in John Kirton and Madeline Koch, eds., G20 Japan: The 2019 Osaka Summit (London: GT Media), pp. 104-105. https://www.globalgovernanceproject.org/g20-performance-on-health/.
Lauren Millar is senior advisor and team lead on global health law and policy at the Global Governance Program, based at the Munk School of Global Affairs and Public Policy at Trinity College in the University of Toronto. She received her J.D. from the University of Ottawa Faculty of Law (exchange at the University of Hong Kong) and her Honours B.A. with High Distinction from Trinity College at the University of Toronto. Lauren is an alumna of the Ontario Legislature Internship Programme and was a Canadian Constitution Foundation Fellow. She has worked in politics, in the government relations department of one of Canada's largest banks and as a litigation associate at a national law firm. Lauren was a researcher with the G8 and G20 Research Groups from 2010 to 2013, and was a member of the field teams for the 2011, 2012 and 2013 summits.
The views and analysis reflected in this article are solely those of the author.
 — 
|
This Information System is provided by the University of Toronto Libraries and the G7 Research Group at the University of Toronto. |
|
Please send comments to:
g7@utoronto.ca This page was last updated December 03, 2020. |
All contents copyright © 2024. University of Toronto unless otherwise stated. All rights reserved.