
Summits | Meetings | Publications | Research | Search | Home | About the G7 Research Group

|
Summits | Meetings | Publications | Research | Search | Home | About the G7 Research Group |
|
G7 Global Fund Commitments, Compliance and Financial Contributions, 2001–2021
Lauren Millar, Senior Advisor, G7 and G20 Research Groups
April 16, 2021
I am grateful for the data and analysis provided by members of the G7 Research Group.
The Group of Seven (G7) major market democracies and the Group of 20 (G20) systemically significant states are both soft law bodies made up of Group of Seven (G7) countries pledge and contribute significant amounts of money annually to international health organizations and initiatives. These commitments are often made or reaffirmed at annual G7 summits. But how well do G7 members comply with them? Is there a connection between a G7 summit directly referencing a specific international health organization in the leaders' commitments, the G7's compliance with that commitment and the amount of G7 financial contributions to that health organization that year? For the purposes of this article, since the G7/8 includes the European Union as a full member, references to compliance and commitments in this article include the EU. however, references to funding allocations do not include the EU, as funding was calculated on a per country basis (i.e., Canada, France, Germany, Italy, Japan, United Kingdom and United States). Similarly, Russia participated in the summits up to and including the 2013 Lough Erne Summit but is excluded from the funding allocations here.This analysis focuses on the Global Fund to Fight AIDS, Tuberculosis and Malaria, among the many international organizations referenced regularly in G7 summit commitments. This international organization provides an excellent case study because of the frequency it is referred to by the G7 in its commitments, the G7 Research Group's compliance analyses of health commitments since 2001 and the Global Fund's reliable, available historical financial data. Moreover, the Global Fund was created by the G7, first discussed at the G7's Okinawa Summit in 2000 and launched the following year at Genoa.This research report finds that from 2001 to 2020, G7 summits complied with their eight assessed Global Fund commitments at an average of 83%, well above the average of 76% compliance for all their health commitments since 1983. G7 compliance with Global Fund commitments steadily rose through three phases, from 78% from 2001 to 2005, to 87% from 2006 to 2007, to 88% from 2016 to 2016. This rise coincides with the general rise in G7 funding for the Global Fund during this time.The G7 summits seemed to strongly, directly support the newly created Global Fund in its early years to meet the proliferating HIV/AIDS crisis raging then. It then turned its attention to other health priorities, using periodic replenishments rather than G7 summits to replenish the fund. A higher number of Global Fund commitments made at G7 summits coincides with increased Global Fund financing from G7 countries. More references are made by the G7 in the last year of a Global Fund financial cycle, but they decrease once funding is secured. However, more data and analysis are needed to confirm these findings and to see if the historic pattern continues during the great crisis that COVID-19 has now brought.
The Global Fund serves as a financing mechanism for AIDS, tuberculosis and malaria prevention, treatment and care programs. The idea of creating it was discussed at the 2000 G8 summit in Okinawa, Japan. In 2001 United Nations secretary general Kofi Annan called for the formal creation of a Global Fund. The G8 officially endorsed its creation at the 2001 Genoa Summit. In that summit's communiqué, all eight countries committed $1.3 billion, asked other countries to contribute, and called on the public and private sectors to play a role. The Global Fund's largest contributors have historically been many of the G7 countries.
The pledges and contributions to the Global Fund usually run on three-year funding cycles. These cycles started in 2001, 2005, 2007, 2010, 2013, 2016 and 2019. Figure 1 illustrates the G7's collective contributions.
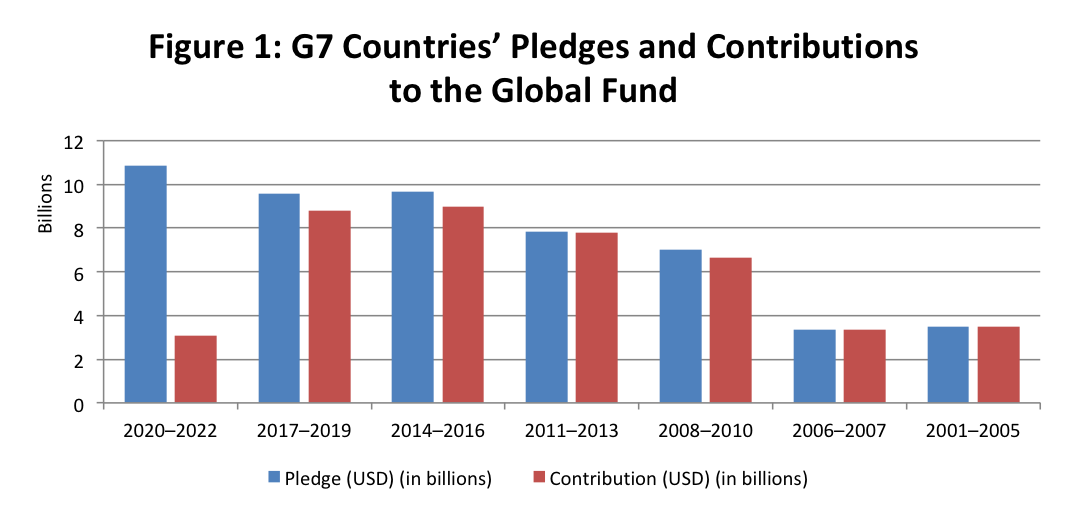 Source: Global Fund Data Explorer, accessed on April 12, 2021. Note: Does not include Russia or the European Union. |
Data from the Global Fund website show that both pledges and contributions have increased dramatically during the 20 years since the Global Fund's start. The largest increase came from the 2006–2007 funding cycle and 2008–2010 funding cycle. Did G7's Global Fund commitments and compliance coincide with this rise and the levels reached during the six three-year funding cycles so far?
At the 2001 Genoa Summit, where the Global Fund was first endorsed and publicly supported by the G8 members, two of the three health-related commitments made there referred specifically to the Global Fund (see Appendix A). Of these two, one was assessed for compliance by the G7 Research Group. This commitment recognized the Global Fund and encouraged active participation of donors in bilateral and multilateral efforts. Overall compliance with this commitment averaged +0.75 or 88%, with the United States and Japan both complying at 50%. In 2002, at the Kananaskis Summit, two commitments were made that directly referenced the Global Fund (see Appendix A). One commitment referencing the Global Fund was assessed for compliance. It encouraged continued support to ensure that the fund continued to increase the effectiveness of its operations and learned from its experience. G8 compliance with this commitment was only +0.25 or 63%. Only Canada, the G8 summit host in 2002 and Italy, which hosted the year before, complied fully, at 100%. In 2003 at Evian, G8 leaders made one commitment to the Global Fund that the G8 Research Group assessed. Here the G8 reaffirmed its commitment to the Global Fund. Compliance increased to +0.89 or a new high of 95%. All members but Germany achieved +1.00 or 100%.At the Sea Island Summit in 2004, one commitment referencing the Global Fund was made (see Appendix A). At the Gleneagles Summit in 2005, with its priority on AIDS, one Global Fund commitment was made and assessed. It included replenishing the fund financially. Compliance was only +0.33 or 67%. Italy was now the outlier with 0%. Therefore, in the first five years of the fund, compliance ebbed and flowed. During this first phase, G8 compliance, with its four assessed Global Fund commitments, averaged 78%. G8 financial pledges and contributions were relatively modest, at $3,473,350,023, but contributions pledged were contributions made in full.
The short phase from 2006 to 2007 started with the G8's 2006 St. Petersburg Summit, with health as one of its three priorities. The G8 specifically referenced the Global Fund in four commitments (see Appendix A). The one assessed Global Fund commitment secured compliance of +0.56 or 78%.The 2007 G8 summit at Heiligendamm made five commitments that directly referenced the Global Fund (see Appendix A). The two assessed for compliance achieved 92%. The first recognized that the demands on the Global Fund would increase substantially in the coming years and that funding would have to increase. G8 members agreed to prioritize working with donors to replenish the fund to provide for longer-term predictable funding. Compliance averaged +0.67, or 84%.The second assessed commitment recognized the growing feminization of the AIDS epidemic and promoted a gender-sensitive response to be included in the Global Fund's efforts. It secured compliance of +1.00, or 100%.This phase includes summits where the Global Fund was directly referenced more than any other time in history. Compliance with the three assessed Global Fund commitments averaged 87%. This was a substantial rise from the 78% compliance in the five-year phase before. In this second phase, G8 financial pledges and contributions to the Global Fund were almost the same as in Phase 1 despite being a much shorter funding cycle. This rise in the number of Global Fund commitments and compliance set the stage for the near doubling in G8 funding in the next phase.
The 2008 summit in Toyako-Hokkaido made no health-related commitments specifically referring to the Global Fund (see Appendix A). This was possibly because of the new funding cycle had started, meaning funds were already secured. At the L'Aquila Summit in 2009, again, no commitments directly referenced the Global Fund (see Appendix A).By 2010, there was an urgent call for new funding by UNAIDS and others. These groups warned of an impending deficit and the need for an increase in funding for programs in 2011–2013 or multiple programs would have to be cancelled. The G8's Muskoka Summit in 2010 focused on its centrepiece of mobilizing money for maternal, newborn and child health, the two of the eight Millennium Development Goals that with the furthest from being met. It raised $7.3 billion in support of the issue and spurred the UN leaders in September to raise this to $40 billion. This left little time to make commitments on the Global Fund.
The fourth phase, from 2011 to 2013, began with the G8 summit in Deauville making a short recommitment to supporting the Global Fund. Yet G8 summits in 2012 and 2013 made no references to the Global Fund (see Appendix A). During this time, the Global Fund's fears came true, and funding was halted due to insufficient funds and calls for reform. It is possible that global leaders did not want to draw attention to what could have looked like a failure. However, out of that crisis, a new, stronger funding model was constructed, which focused on strategic investments requiring scientific evidence, and in return receiving more predictable funding. Other global health issues were hardly discussed at the G8 summits in 2012 and 2013. They produced the fewest health commitments of any summit since 1993: just one at Camp David in 2012 and two at Lough Erne in 2013. These years reflect one of the periods of the lowest G8 focus on global health, correlating with the smallest overall funding increases to the Global Fund during this phase from the one before.
Although the Global Fund's financial issues were not raised at the G8 summit in 2013, the largest amount ever was committed to fighting these three diseases through the fund came for the 2014–2016 period, using the new funding formula.In 2016, at Ise-Shima a Global Fund commitment was again assessed by the G7 Research Group. Here G7 members (now without Russia) committed to "ending AIDS, tuberculosis and malaria, working in partnership with the Global Fund … and others." It secured high compliance +0.75 or 88%. Only the United Kingdom received a score of 0.In stark contrast to previous summits, the Ise-Shima Summit focused on health. It made 85 health commitments, the highest in G7 history (see Appendix B). Five referred to the Global Fund (see Appendix A). Yet the G7 largely focused on other global health crises, such as the Ebola pandemic. It is possible that because of this, and because of the need for scarce resources to address multiple health crises, there was a drop in funding between this funding cycle and the next one. Moreover, the diversionary effect of acute outbreak events taking attention and funding away from the chronic and now more controlled Global Fund diseases is consistent with the fact that in this phase and the next, G7 countries provided less funding than they had pledged.
During the sixth phase, from the Taormina Summit in 2017 to the Biarritz Summit in 2019, the G7 made very few overall health commitments, with seven made in 2017, nine in 2018 and four in 2019 (see Appendix B). In 2017, no commitments referenced the Global Fund. In 2018, one referenced the fund and in 2019 three referenced it (see Appendix A). However, none of these commitments was assessed for compliance.This funding cycle was the first since the Global Fund's inception that funding decreased overall from G7 countries, if only a little.
The seventh phase, from 2020 to 2022, started with the G7's health attention and action largely crowded out by the COVID-19 crisis. The crisis dominated the many health commitments made at the emergency G7 summit on March 16, 2020, and the virtual summit held on February 19, 2021.Yet this cycle began with the largest amount ever raised for the Global Fund in 2019 for the period 2020-2022. All G7 countries, except Japan, increased their commitments by at least 15%. These pledges, however, were made before the COVID-19 crowd-out came. Time will tell whether countries are able and willing to contribute the full amount pledged. While the G7's attention focuses almost entirely on health-related issues, the issue of COVID-19 in particular may negatively affect the amount of resources being invested into preventing AIDS, tuberculosis and malaria. Yet the COVID-19 crisis could spur action on health as a whole, with a focus on primary health care, vaccination and even universal health coverage.
From 2001 to 2020, G7 summits complied with their eight assessed Global Fund commitments at an average of 83%. This is well above the average of 76% for all the 73 assessed health commitments they made since 1983 (see Appendix B).The limited compliance data available for the G7's Global Fund commitments suggest it steadily rose through three phases, from 78% during the first phase from 2001 to 2005, to 87% during the second phase from 2006 to 2007, to 88% during the fifth phase from 2014 to 2016. This rise coincides with the general rise in G7 funding for the Global Fund during this time.More compliance data are needed to see if a tighter correlation data exists. At present, it seems that the G7 provided strong direct summit support in the early years to get its newly created Global Fund off the ground, to meet the proliferating HIV/AIDS crisis raging then. It then turned its attention and funding to other health priorities, such as maternal, newborn and child health and Ebola, using periodic replenishments to support the fund.Although it is unclear whether the amount of financial contributions made by the G7 annually has an impact on compliance with Global Fund commitments, it seems likely that a higher number of Global Fund commitments made at G7 summits coincides with more Global Fund financing from the G7. The number increases in the last year of a Global Fund financial cycle and decreases once funding is secured. It will be important to continue to track the Global Fund, to determine the impact of COVID-19 pandemic, and whether this pandemic will drive resources away from deadly epidemics and pandemics that the G7 have been fighting for decades.
| Summit | Global Fund Commitments |
| 2000 Okinawa | No commitments made. |
| 2001 Genoa | 2001-26. To meet that commitment and to respond to the appeal of the UN General Assembly, we have launched with the UN Secretary-General a new Global Fund to fight HIV/AIDS, malaria and tuberculosis. We are determined to make the Fund operational before the end of the year. We have committed $1.3 billion. 2001-27. In the context of the new Global Fund, we will work with the pharmaceutical industry and with affected countries to facilitate the broadest possible provision of drugs in an affordable and medically effective manner. |
| 2002 Kananaskis | 2002-119. Continuing support for the Global Fund to Fight AIDS, Tuberculosis and Malaria, and working to ensure that the Fund continues to increase the effectiveness of its operations and learns from its experience. 2002-120. Supporting African efforts to increase Africa's access to the Global Fund and helping to enhance Africa's capacity to participate in and benefit from the Fund. |
| 2003 Evian-les-Bains | 2003-10. We agreed on measures to strengthen the Global Fund to fight AIDS, Tuberculosis and Malaria and other bilateral and multilateral efforts, notably through our active participation in the donors' and supporters' conference to be hosted in Paris this July. 2003-113. We reaffirm our support for the Global Fund to fight AIDS, Tuberculosis, and Malaria. 2003-114. We welcome and support the proposal to host, in collaboration with the Global Fund, an international donors' and supporters' conference bringing together governments, international organisations, NGOs [non-governmental organizations] and members of the private sector active in this field in Paris in July. |
| 2004 Sea Island | No commitments made. |
| 2005 Gleneagles | 2005-72: We will work to meet the financing needs for HIV/AIDS, including through the replenishment this year of the Global Fund to fight AIDS, TB [Tuberculosis] and Malaria; and actively working with local stakeholders to implement the '3 Ones' principles in all countries. |
| 2006 St. Petersburg | 2006-4: fulfillment of prior G8 commitments on the major infectious diseases, in particular by mobilizing support for the Global Fund to Fight AIDS, Tuberculosis, and Malaria; continuing to pursue as close as possible to universal access to HIV/AIDS treatment for all who need it by 2010; supporting the Global Plan to Stop TB; providing resources in cooperation with African countries to scale up action against malaria; continuing to expand the Global HIV Vaccine Enterprise; and continuing our support for the Global Polio Eradication Initiative so that the planet can be declared polio-free within the next few years. 2006-24: We pledge our continued support to the Joint United Nations Programme on HIV/AIDS (UNAIDS), the WHO [World Health Organization], the Global Fund to fight AIDS, Tuberculosis and Malaria (the Global Fund), the World Bank and other organizations, initiatives and partnerships actively working to fight these diseases. 2006-32: The G8 members will work with governments and technical agencies to support the preparation of high quality, timely proposals for Global Fund AIDS, Tuberculosis and Malaria grants. 2006-312: We reaffirmed our commitments to fight HIV/AIDS, tuberculosis and malaria and agreed to work further with other donors to mobilize resources for the Global Fund to Fight AIDS, Tuberculosis and Malaria and to continuing to pursue as closely as possible to universal access to HIV/AIDS treatment for those who need it by 2010. |
| 2007 Heiligendamm | 2007-227: [We recognize that the level of demand to the Global Fund to fight AIDS, Tuberculosis and Malaria (GFATM) will increase substantially in the future as has been projected by the GFATM Board. In this regard, noting the conclusions of the April meeting of the GFATM Board, which estimated an additional demand approximately of US$ 6 billion by 2010 which might possibly reach US$ 8 billion,] G8 members pledge to work with other donors to replenish the GFATM and to provide long-term predictable funding based on ambitious, but realistic demand-driven targets. 2007-228: G8 partners will work with other stakeholders so that Global Fund resources continue to be used in alignment with existing national priorities and processes. 2007-229: Recognizing the growing feminization of the AIDS epidemic, the G8 in cooperation with partner governments support a gender-sensitive response by the GFATM, with the goal of ensuring that greater attention and appropriate resources are allocated by the Fund to HIV/AIDS prevention, treatment, and care that addresses the needs of women and girls. 2007-247: We will therefore work with UNAIDS, WHO, WB [World Bank] and the GF [Global Fund] to strengthen their efforts and work together with the African Union and African States, the innovative and generic pharmaceutical industry, private donors, civil society and other relevant stakeholders to help deliver next steps towards "universal access". 2007-251: [In particular we will work with: African Governments] to develop country-led policies that can ensure effective coordination of donor health programs and identify technical assistance needs, with the support of the WHO, World Bank, UNAIDS, GFATM and other agencies. |
| 2008 Hokkaido-Toyako | No commitments made. |
| 2009 L'Aquila | No commitments made. |
| 2010 Muskoka | 2010-15: We will support country-led efforts to achieve this objective by making the third voluntary replenishment conference of the Global Fund to Fight AIDS, TB and Malaria in October 2010 a success. |
| 2011 Deauville | 2011-62: We will continue to support the Global Fund to Fight AIDS, Tuberculosis and Malaria. |
| 2012 Camp David | No commitments made. |
| 2013 Lough Erne | No commitments made. |
| 2014 Brussels | 2014-95: [We reaffirm our commitment to] the Global Fund to fight AIDS, Tuberculosis and Malaria to reduce the burden of these three major infectious diseases on eligible countries and regions. |
| 2015 Elmau | No commitments made. |
| 2016 Ise-Shima | 2016-80: We are committed to ending AIDS, tuberculosis and malaria, working in partnership with the Global Fund (GF) and others. 2016-81: To this end, we fully support a successful 5th replenishment of the GF, taking the opportunity of the GF replenishment conference in Montreal in September, and call on traditional and new donors to support the replenishment. 2016-207: With this in mind and recognizing the pressing need for strong, resilient and sustainable health systems in Low Income Countries (LICs) and Lower Middle Income Countries (LMICs) with limited resources and increased vulnerability to public health threats such as epidemic and other severe events, commit to support country-led HSS [health system strengthening] with greater use of enhanced coordination of country-level actions toward HSS, based on the IHP+ [International Health Partnership] principles, including through the Country Coordination Mechanism of the Global Fund, as well as the GHSA [Global Health Security Agenda]. 2016-216: Also fully support a successful 5th replenishment of the Global Fund (GF), which plays a major role in reducing the impact of significant infectious diseases as well as promoting HSS, taking the opportunity of the GF replenishment conference in Montreal in September this year, and also call on all traditional and new donors to support the GF achieve its goals and on all countries to increase their domestic resources for health. 2016-229: Support the work of global partnerships such as the Global Fund to Fight AIDS, Tuberculosis and Malaria, Gavi the Vaccine Alliance, the Global Alliance for Chronic Diseases, and UHC 2030 building upon IHP+, as well as global initiatives such as the implementation of the Global Strategy for Women's, Children's and Adolescents' Health and the GFF [Global Financing Facility for Every Women Every Child] as appropriate. |
| 2017 Taormina | No commitments made. |
| 2018 Charlevoix | 2018-26: We affirm our support for a successful replenishment of the Global Fund in 2019. |
| 2019 Biarritz | No commitments made. |
| Summit | Domestic political management | Deliberation | Direction setting | Decision making | Delivery | Development of global of governance | ||||||||||
| # compliments | % compliments | Words | Documents | Priority placement | Democracy | Human rights | # made | # assessed | % assessed | Score | % | Inside | Outside | |||
| # | % | # references | #bodies | |||||||||||||
| 1975 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | - | - | - |
| 1976 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | - | - | - |
| 1977 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | - | - | - |
| 1978 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | - | - | - |
| 1979 | 0 | 0 | 15 | 0.7 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1980 | 0 | 0 | 116 | 2.9 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1981 | 0 | 0 | 59 | 1.8 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1982 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1983 | 0 | 0 | 21 | 0.97 | 1 | 0 | 0 | 0 | [0] | 1 | ? | +1.00 | 100% | 0 | 0 | 0 |
| 1984 | 0 | 0 | 12 | 0.36 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1985 | 0 | 0 | 59 | 1.8 | 2 | 0 | 1 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1986 | 0 | 0 | 74 | 2 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1987 | 1 | 50% | 719 | 14 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 2 | 1 |
| 1988 | 1 | 33% | 195 | 4 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1989 | 0 | 0 | 272 | 3.8 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 5 | 4 |
| 1990 | 0 | 0 | 146 | 1.9 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 1 | 1 |
| 1991 | 0 | 0 | 300 | 3.7 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 3 | 3 |
| 1992 | 0 | 0 | 34 | 0.45 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1993 | 0 | 0 | 62 | 1.8 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 1 | 0 | 0 |
| 1994 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1995 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 0 | 0 | 0 |
| 1996 | 0 | 0 | 825 | 5.3 | 2 | 0 | 0 | 0 | 3 | 0 | n/a | n/a | n/a | 0 | 9 | 7 |
| 1997 | 0 | 0 | 1,400 | 10.7 | 2 | 0 | 1 | 1 | 4 | 0 | n/a | n/a | n/a | 1 | 6 | 4 |
| 1998 | 0 | 0 | 404 | 6.6 | 1 | 0 | 0 | 0 | 4 | 3 | 75% | +0.36 | 68% | 0 | 5 | 5 |
| 1999 | 0 | 0 | 589 | 5.8 | 2 | 0 | 0 | 0 | 3 | 1 | 33% | 0 | 50% | 0 | 6 | 5 |
| 2000 | 0 | 0 | 1,996 | 14.6 | 2 | 0 | 0 | 0 | 14 | 5 | 36% | +0.82 | 91% | 1 | 25 | 7 |
| 2001 | 0 | 0 | 1,520 | 24.4 | 2 | 0 | 0 | 0 | 3 | 2 | 66% | +0.88 | 94% | 2 | 21 | 7 |
| 2002 | 0 | 0 | 1,482 | 12.3 | 2 | 0 | 0 | 0 | 18 | 8 | 44% | +0.43 | 72% | 0 | 2 | 1 |
| 2003 | 0 | 0 | 3,753 | 22.2 | 3 | 0 | 0 | 0 | 15 | 6 | 40% | +0.80 | 90% | 2 | 29 | 16 |
| 2004 | 0 | 0 | 1,507 | 3.9 | 3 | 0 | 0 | 0 | 9 | 2 | 22% | +0.50 | 75% | 0 | 7 | 7 |
| 2005 | 0 | 0 | 2,197 | 9.8 | 4 | 0 | 0 | 0 | 11 | 6 | 55% | +0.44 | 72% | 0 | 7 | 6 |
| 2006 | 2 | 40% | 7,072 | 23 | 7 | 0 | 0 | 1 | 60 | 5 | 8% | +0.37 | 69% | 0 | 63 | 16 |
| 2007 | 0 | 0 | 4,263 | 16.4 | 4 | 0 | 0 | 6 | 42 | 6 | 14% | +0.71 | 86% | 0 | 50 | 17 |
| 2008 | 0 | 0 | 2,008 | 11.9 | 3 | 0 | 0 | 0 | 19 | 4 | 21% | +0.17 | 59% | 0 | 8 | 5 |
| 2009 | 0 | 0 | 2,338 | 14 | 6 | 0 | 1 | 4 | 9 | 3 | 33% | +0.37 | 69% | 0 | 21 | 11 |
| 2010 | 0 | 0 | 2,772 | 26.1 | 1 | 0 | 0 | 2 | 12 | 4 | 33% | +0.14 | 57% | 0 | 22 | 13 |
| 2011 | 1 | 10% | 756 | 4.1 | 2 | 0 | 0 | 0 | 7 | 1 | 14% | −0.11 | 45% | 0 | 10 | 6 |
| 2012 | 0 | 0 | 450 | 12.3 | 1 | 0 | 2 | 5 | 1 | 1 | 100% | +1.00 | 100% | 0 | 1 | 1 |
| 2013 | 0 | 0 | 934 | 6.92 | 2 | 0 | 0 | 0 | 2 | 1 | 50% | +0.89 | 95% | 0 | 5 | 5 |
| 2014 | 1 | 20% | 446 | 8.7 | 1 | 0 | 0 | 2 | 12 | 3 | 25% | +0.83 | 92% | 0 | 3 | 2 |
| 2015 | 1 | 14% | 2,190 | 17.3 | 2 | 0 | 0 | 1 | 61 | 3 | 5% | +0.71 | 86% | 0 | 23 | 12 |
| 2016 | 5 | 23% | 6,087 | 26.4 | 2 | 0 | 0 | 25 | 86 | 3 | 3% | +0.50 | 75% | 3 | 65 | 15 |
| 2017 | 0 | 0 | 885 | 10.2 | 2 | 0 | 0 | 2 | 7 | 1 | 14% | −0.50 | 25% | 1 | 3 | 3 |
| 2018 | 0 | 0 | 713 | 6.3 | 2 | 0 | 0 | 1 | 9 | 1 | 11% | +0.50 | 75% | 0 | 3 | 3 |
| 2019 | 0 | 0 | 1,145 | 15.9 | 0 | 0 | 1 | 1 | 4 | n/a | n/a | n/a | n/a | 1 | 4 | 4 |
| 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 12 | 49,816 | 355.3 | 76 | 0 | 7 | 51 | 415 | 70 | 12 | 409 | 187 | ||||
| Average | 0.3 | 0.0 | 1,107 | 7.9 | 1.7 | 0 | 0.2 | 1.1 | 9.4 | 1.6 | 0.2% | +0.50 | 75% | 0.3 | 10.0 | 4.6 |
Notes:
All data derived from documents issued in the G7/8 leaders' names at each summit. n/a = not available. Compiled by Brittaney Warren, December 19, 2020.
Domestic political management includes all communiqué compliments related to health, i.e., references by name to the G7/8 member(s) that specifically express gratitude in the context of health. % indicates how many G7/8 members received compliments in the official documents, depending on the number of full members participating.
Deliberation refers to the number of references to health. The unit of analysis is the paragraph. % refers to the percentage of the words in each document that relate to health.
Direction setting: priority placement refers to the number of references to health in the chapeau or chair's summary; the unit of analysis is the sentence. Democracy refers to the number of references to democracy in relation to health. Human rights refers to the number of references to human rights in relation to health.
Decisions made refers to the number of health commitments made. Decisions assessed refers to the number and percentage of health commitments assessed of the total made.
Delivery refers to the overall compliance score for health commitments measured for that year. % assessed refers to percentage of commitments measured.
Development of global governance: inside refers to the number of references to G7/8 health ministers; outside refers to the number of multilateral organizations related to health. The unit of analysis is the sentence.
Lauren Millar is senior advisor and team lead on global health law and policy at the Global Governance Program, based at Trinity College in the University of Toronto. She received her J.D. from the University of Ottawa Faculty of Law (exchange at the University of Hong Kong) and her Honours B.A. with High Distinction from Trinity College at the University of Toronto. Lauren is an alumna of the Ontario Legislature Internship Programme and was a Canadian Constitution Foundation Fellow. She has worked in politics, in the government relations department of one of Canada's largest banks and as a litigation associate at a national law firm. Lauren was a researcher with the G8 and G20 Research Groups from 2010 to 2013, and was a member of the field teams for the 2011, 2012 and 2013 summits.The views and analysis reflected in this article are solely those of the author.
 — 
|
This Information System is provided by the University of Toronto Libraries and the G7 Research Group at the University of Toronto. |
|
Please send comments to:
g7@utoronto.ca This page was last updated August 15, 2024. |
All contents copyright © 2026. University of Toronto unless otherwise stated. All rights reserved.